
Case 68: Identifying the Correct Matrix on Radiographs
37-years old presented with a knee swelling

Case:
37-years old presented with a knee swelling. Only films were available for review.
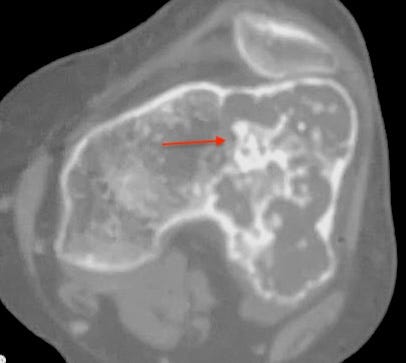
The radiograph shows an expansile osteolytic lesion in the distal femur with thinning of the anterior cortex with a narrow zone of transition without periosteal reaction or cortical break, epimetaphyseal and extending into the diaphysis (Fig. 1).


This suggests a slow-growing, perhaps benign or low grade malignant lesion.
An epi-metaphyseal, juxtamedullary lesion in this age group should trigger a diagnosis of giant cell tumor (GCT), but GCTs rarely have sclerotic rims.
More importantly there is a matrix (arrow in Fig. 1B), which shows a rings and arcs appearance, suggestive of cartilage.
A cartilage tumor like this is too big and eccentric for an enchondroma, though rarely a chondroblastoma or chondromyxoid fibroma could be this big. Both would show marrow edema on MRI presenting as “benign aggressive lesions”. If not, then this is a chondrosarcoma, either Gd 1 or Gd 2.
The CT (Fig. 2) confirms the chondroid matrix.
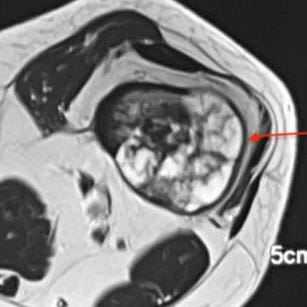
The axial T2 MRI (Figs. 3, 4) shows the typical lobulated septate appearance of a cartilage tumor with no marrow edema on the sagittal STIR (FIg. 5) image.


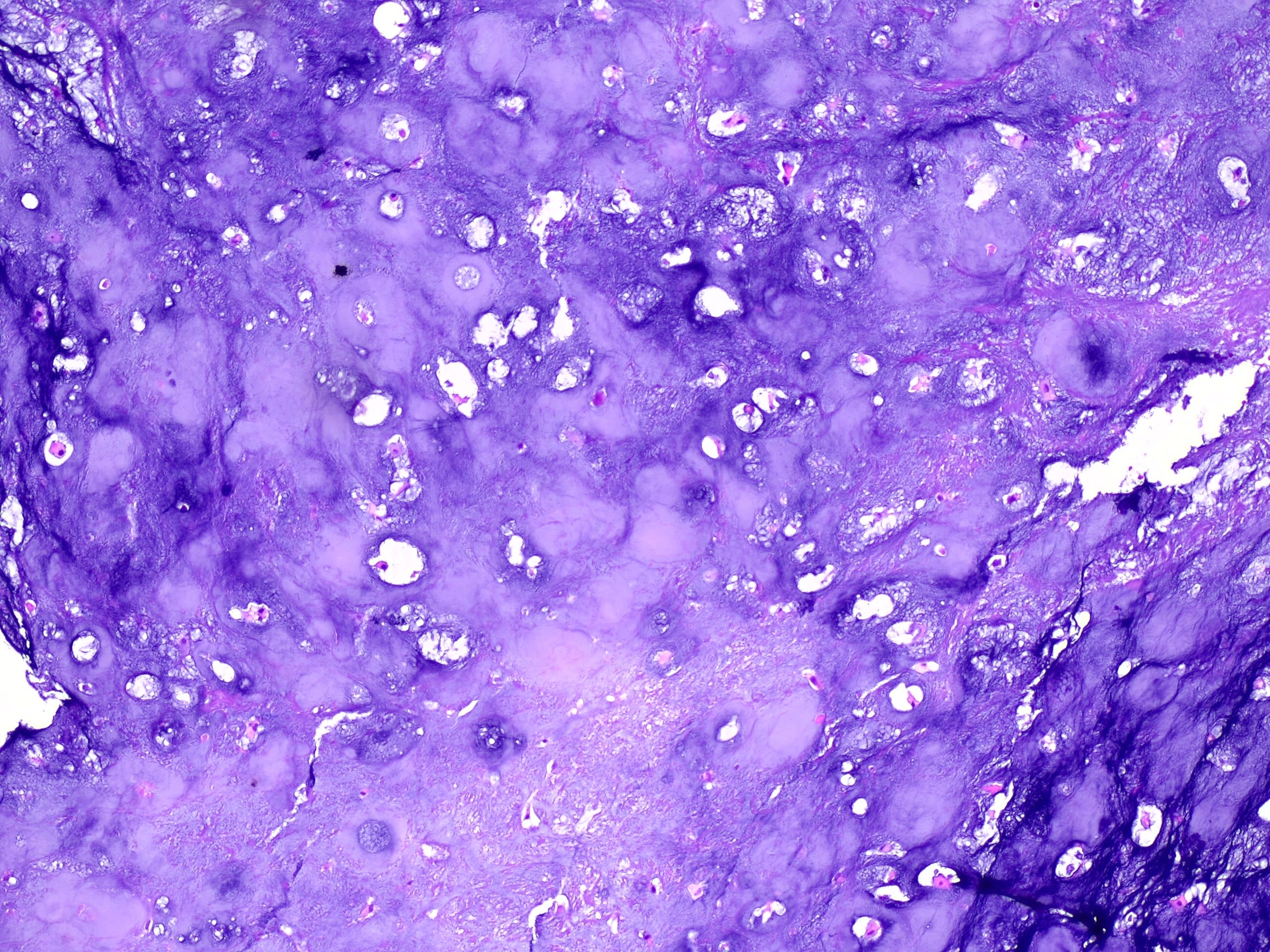
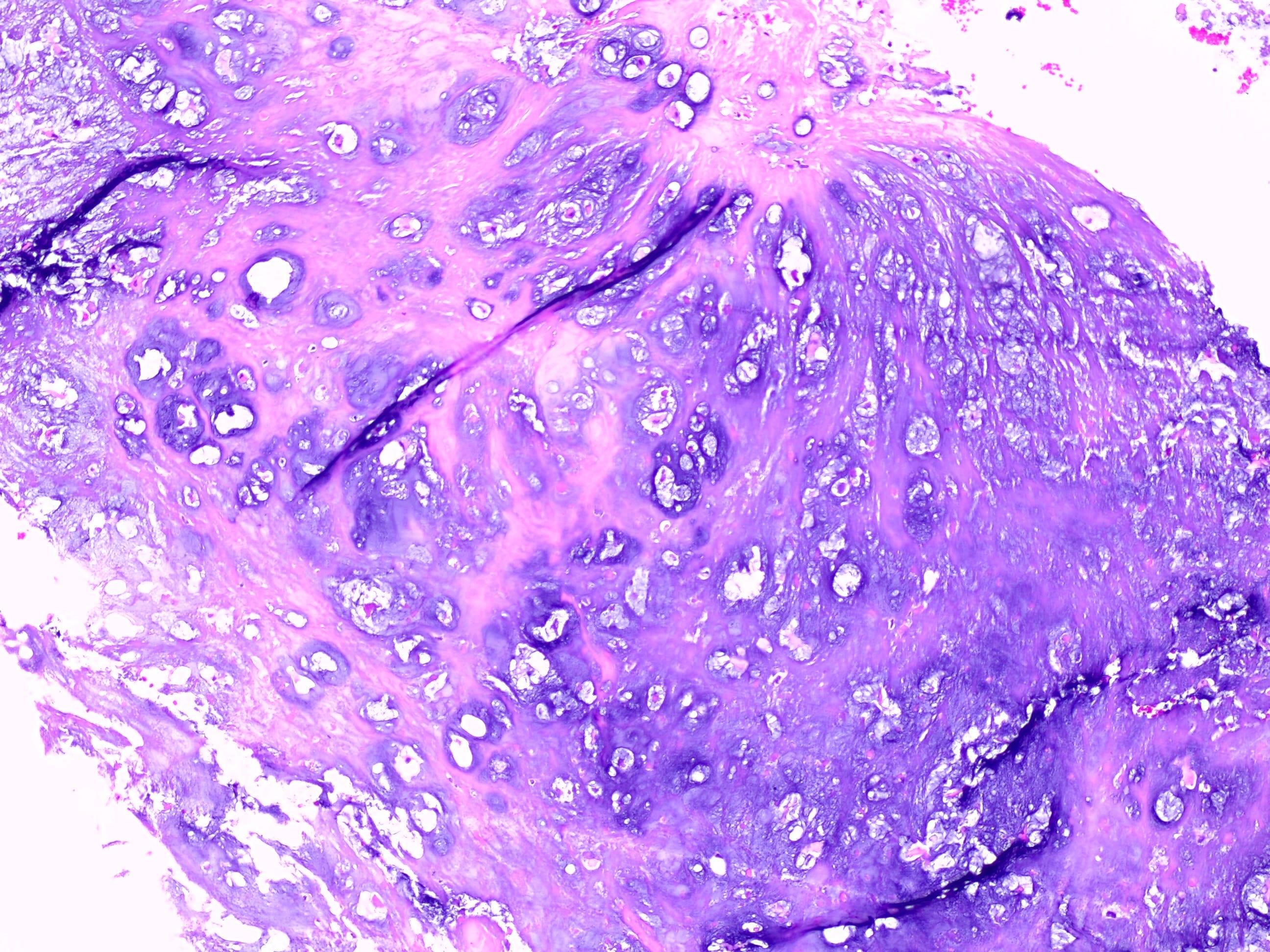
The histopathology (Figs. 6, 7) show a Gd II chondrosarcoma.
A careful perusal of the radiographs often allows us to make a reasonable diagnosis. The MRI then helps confirm and the histopath then validates. Reading an MRI without the radiograph can lead to all sorts of problems
Other Chondrosarcoma cases


Index and Table of Contents

Previous Post
Case 67: Osteochondroma or Chondrosarcoma?

Please subscribe, if you would like to know each time a new post is published
Content So Far
68 Cases
16 Cases of the Day
5 Lectures